The Quarter-Million Dollar Blindspot: Micro-Aversions vs. Macro-Gains in SNF Operations
Carrying the weight of a skilled nursing facility’s public reputation, survey compliance, and fiscal health is an exhausting, high-stakes balancing act. Too often, MDS coordinators find themselves marooned on “MDS Island”—treated like a “fake paper nurse” by bedside staff, yet held solely accountable by corporate leadership the moment frontline documentation fails to support the financial grid. Meanwhile, Administrators and Directors of Nursing face immense stress over survey tags, regulatory confusion, and sudden financial leaks.
As we look at regional audit trends and large-scale clinical reviews across the sector this quarter, a striking operational paradox stands out.
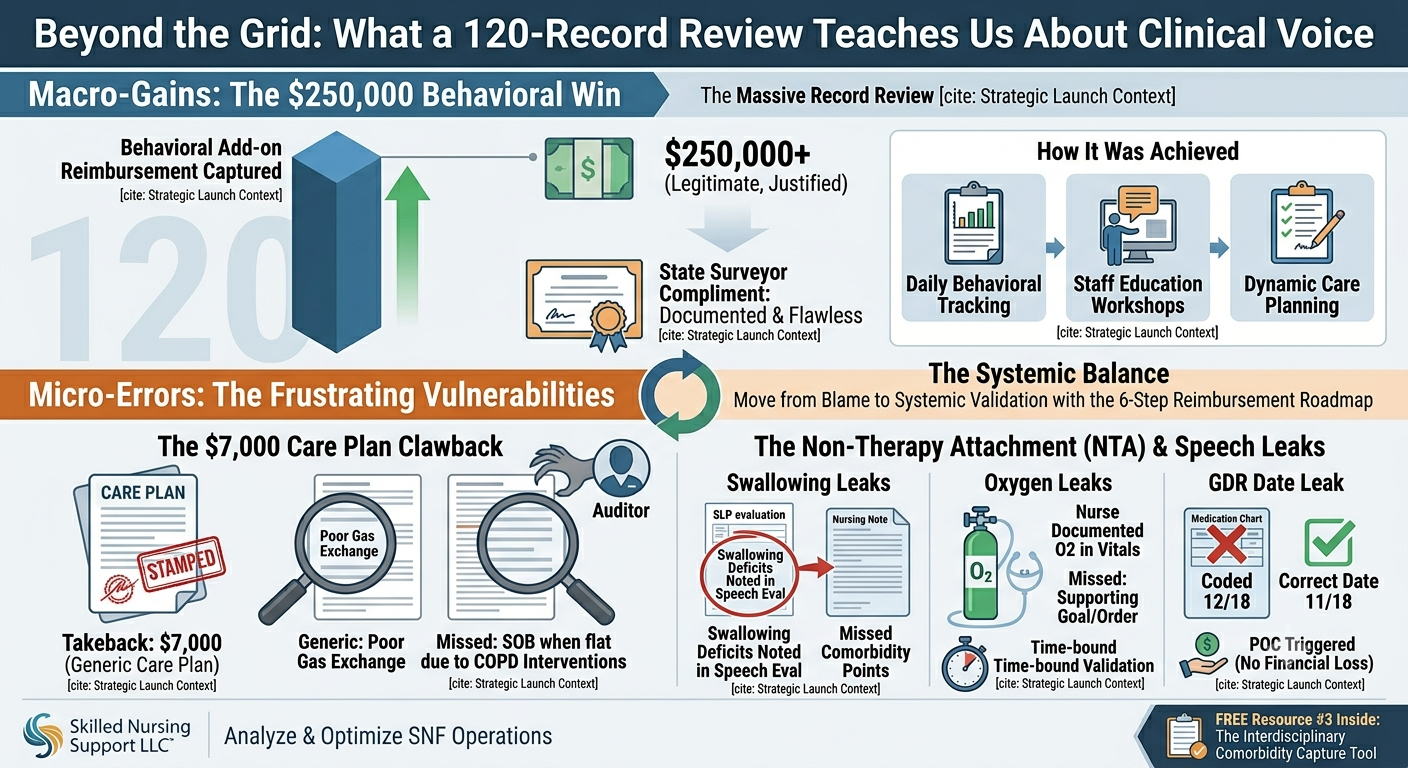
Across the industry, we are seeing clinical teams pull off incredible operational victories. Through diligent daily tracking, robust behavioral care planning, and staff education, high-performing coordinators are successfully capturing upwards of $250,000 in legitimate behavioral add-on reimbursement. In many cases, state auditors are publicly complimenting the exceptional depth of these behavioral tracking systems.
Yet, inside these exact same regional reviews, a frustrating pattern emerges: these massive quarter-million-dollar wins are frequently overshadowed by minor, technical administrative oversights.
For example, regulatory data shows a spike in retroactive insurance clawbacks simply because a resident with documented respiratory interventions (like shortness of breath when lying flat) was care-planned under a generic symptom like “poor gas exchange” without an explicit, structural link to the underlying medical diagnosis like COPD. Combine that with simple, single-digit date typos on antipsychotic Gradual Dose Reduction (GDR) tracking sheets, and a facility faces an administrative Plan of Correction (POC) over a clerical error, despite outstanding clinical care.
When technical documentation gaps trigger financial losses or survey flags, the common corporate reflex is to treat it as an individual staff failure. But after more than three decades serving as a floor nurse, DON, and Regional Corporate Reimbursement Manager, I know that technical leaks are rarely a clinical capability or training problem—they are an operational framework problem.
The True Cost of the “Legwork” Bottleneck
Missing a single clinical driver or failing to validate an underlying comorbidity code isn’t just an administrative oversight—it equates to letting an incredibly complex resident live in your building for free, costing upwards of $100,000 a year.
When structural leaks occur, they usually happen in three silent interdisciplinary bottlenecks:
-
The Buried SLP Note: A Speech-Language Pathology evaluation explicitly notes a swallowing deficit, but because the facility’s interdisciplinary workflow lacks an immediate cross-department alert, those high-value speech comorbidity points never make it to the MDS assessment.
-
The Passive Malnutrition Indicator: Clear clinical signs of malnutrition are sitting inside the dietary logs, but the workflow isn’t structured to prompt an immediate, active physician query before the look-back window slams shut.
-
The Isolated Oxygen Box: Frontline nurses accurately check the box for oxygen use in the daily vitals tracking, but the system fails to prompt the vital next step—validating the active physician order and mapping a compliant, time-bound treatment goal within the care plan.
Systemic Validation Over Reactive Blame
True resident-centered care and accurate fiscal reimbursement are not a game of numbers. They are achieved simultaneously by capturing the resident’s true clinical voice inside the official CMS framework.
When facilities utilize a structured approach like the 6-Step Resident-Centered Reimbursement Roadmap, we bridge the gap between clinical reality and financial compliance. By building an operational safety net around your team, leadership and clinical specialists can work in tandem. You can confidently celebrate and protect your massive financial wins—like robust behavioral tracking—while ensuring the technical care plan details never leave your building vulnerable to an audit.
Take the Next Step: Join My Live Masterclass ??
If you are ready to stop chasing documentation and finally bridge the gap between floor clinical tracking and the financial grid, save your seat for my upcoming live virtual masterclass:
“Unmasking the Chart-to-Grid Disconnect: The 48-Hour PDPM Gatekeeper Protocol” ? Thursday, July 9th, 2026 at 1:00 PM EST
This is a free, high-impact 60-minute session designed specifically for SNF Administrators, DONs, and MDS leaders who want to secure their frameworks and stop compliance bleeding.
[Link: Click Here to Save Your Free Masterclass Seat]
My Gift to You: The Interdisciplinary Comorbidity Capture Tool ?
To help your clinical and leadership teams instantly align your daily documentation with the official framework, I have added a brand-new asset to our subscriber resource library.
This week, you can download Free Resource #3: The 3-Step Verification Protocol for High-Risk Clinical Drivers. This operational sheet gives your team a clear, step-by-step pathway to validate swallowing deficits, active oxygen orders, and physician queries before you submit your data.
[Click Here to Access the Free Resource https://docs.google.com/document/d/1jj81zmdJy4acN9YZfSatUB8fXInEuoPFRDUIOqgfjHc/edit?usp=share_link]
To your compliance and peace of mind,
Maria Messina, RN Founder & Executive Consultant Skilled Nursing Support LLC www.skillednursingsupport.com
P.S. Next month, I’m hosting an ultra-exclusive, intimate chart-auditing sanctuary on the water here in Newburyport, MA to help exactly 4 local leaders reclaim their clinical sanity and master their frameworks. Watch your inbox closely—the registration details drop soon.
Leave a Reply